Ask an expert
Dr. Taqua Dahab
ST9 in Acute, General, and intensive Care Medicine. Special interests in POCUS, Organ Donation, and Medical Education.
Liverpool University Hospital Foundation Trust
Email: Taqua.Dahab1@nhs.net
X : @TaquaDahab

I obtained my primary medical qualification from my home country
of Sudan, and then I moved to the Republic of Ireland to do an equivalence for Core Medical Training. After that, I came to the UK as an ST3 trainee in Acute Medicine—which was my first encounter with the NHS system. After three years in Acute Medicine, I decided to undertake a new adventure and join Intensive Care Medicine in the triple CCTs pathway. I am currently in stage three of the programme, I have a special interests in Point of Care Ultrasound (POCUS) including Echocardiography, I am the Organ Donation Fellow for NHSBT, and have a degree in Medical Education with special interest in Differential Attainments among the International Medical workforce.
What got you interested in Intensive Care Medicine (ICM)?
When I worked as an Acute Med registrar, I enjoyed dealing with the undifferentiated multiorgans sick patients. It fits my personality well as a curious person who tries to solve a puzzle and comes up with problem lists and a probable diagnosis. However, I noted as an Acute Medic, my journey of supporting these patients ends sometimes by admitting them to the door of the Intensive Thearpy Unit (ITU) for more advanced multi-organ support. I always wanted to see what is behind that door…
It was when I had my ITU placement for AIM, I discovered how beautiful this world of ICM is. A highly expert multi-disciplinary team works to provide the best evidence-based medicine to every sick individual at the ITU. From unique Cutting-edge technology in organ support to daily input of POCUS-guided treatment, guided by ongoing clinical research trials, and ending with psychologist support for the survival of the patients and their families, Sometimes, the ends are not always what we hoped for. Still, we manage to support patients and their families in the Organ Donation process to present the gift of life to another sick person in different parts of the country!
Having a snapshot of ITU in a limited placement for AIM strongly convinced me that I needed to follow my passion looking after the undifferentiated multi-organ sick patient from the front door to the ITU door. I rated this as one of the best decisions I have made in my life.
How did you train in ICM?
In ST5, I applied to ICM National Recruitment. This starts every November through the Oriel website. The mandatory requirement to join the ICM training programme from a medical background requires the MRCPUK and an existing National Training Number (NTN) in AIM with the successful most recent ARCP. Interviews follow this in March of every year with questions highlighting commitment to ICM, prioritisation tasks for multiple emergencies you get to expose as an ITU reg, to highlight the leadership skills, clinical scenario, and ethical scenario.
The triple CCT pathways look like this diagram:
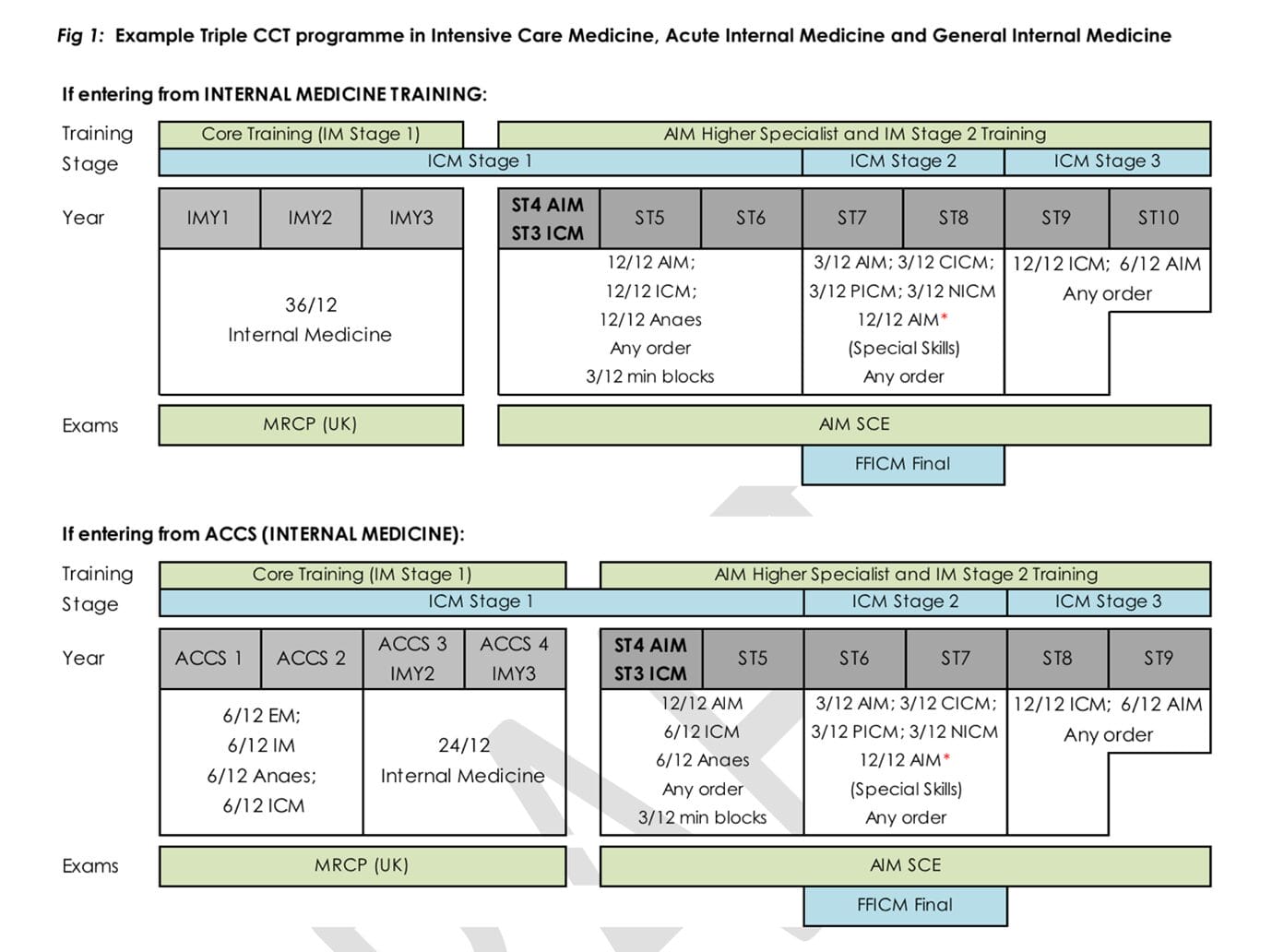
The training programme has three stages.
Stage 1
You will have one year in Acute & General Medicine, Anaesthetics, and ICM.
Stage 2
One year in specialised ITU (Cardiac ITU, Neuro ITU, and Paediatric ITU)
One year in AIM/GIM
Stage 3
One year as an advanced year in ICM
Six months AIM/GIM
You get to spend 32 months in total in AIM/GIM and 48 months in ICM.
You will have to spend a year as a CT1 anaesthetist to have all your airway competencies signed off before moving to the ITU airway registrar rota.
You have to take additional exams on the top of AIM SCE exam. This is a Fellowship exam for the Faculty of Intensive Care Medicine (FFICM). It requires decent preparation and time, it has three components: written, OSCE, and Viva. You must clear this exam before moving to the final year of ICM training. This is the exit exam for the ICM CCT.
Website for triple CCT in AIM/GIM/ICM is here
Were there any challenges?
Both AIM and ICM are ‘generalist’ specialities. They complement each other very well when done well. However, a vast range of knowledge and experience is required to work well in both. Keeping updated with all relevant guidelines, and new EBM requires enthusiasm and effort.
During training, it is often you spend a year in AIM and then move back to ICM. There will be multiple points where your confidence dips when you return to the other speciality after some time away from it. This could often be mitigated by spending in-touch days in the counter speciality and having regular theatre lists in your SPA time to keep up with the airway competencies.
Doing ICM as a triple speciality means that you will have an additional Fellowship exam that needs time, effort, and concentration to pass. You cannot progress to the final year of ICM training without the Fellowship.
How does this fit into your consultant’s work?
Consultants’ job plans vary between regions and trusts. It would help if you negotiated your job plan between the two departments to create a bespoke one. The usual number of Professional Activities (PAs) is 10 to 12. Most AIM/ICM consultants spend 60% to 80% of their time in ITU. The AIM/GIM time is often spent looking after Enhanced Care Areas, but it could be anywhere you like on the AIM floor. You cannot be the on-call consultant for the two specialities simultaneously.
Your job plan may also accommodate if you have any particular interest sessions like teaching, Echo sessions, or leadership roles.
Do you have any tips for Intensive Care Medicine triple CCT trainees?
If you knew early that you wanted to triple CCT, applying early for the second NTN is advisable to fit nicely in the three stages of training discussed above. Follow the FICM website’s calendar for events, courses, and conferences that could be helpful to attend and participate in. It will show commitment to ICM when you apply and buff your application score.
Exams are often not a pleasant time; try to clear AIM SCE and FFICM as early as possible so that you can enjoy your training relatively stress-free and have special interests toward the end of your training,
POCUS is a mutual shared skill for both AIM and ICM; you may need to love your Ultrasound probe more, as you will need to use it daily, this will include your FAMUS curriculum as well as learning basic Echo skills (Echo is optional in ICM, but very recommended).